|
|
 Electrode Array Electrode Array
|
There are a lot of people which lost their arms or legs, some people lost them because of war or accidents, others are affected by down syndrome. However, there is a kind of new technology called robotic limb which could let them live a normal life. The structure of the robotic limb can be divided into two parts, one is mechanical and the other one is control system.
Today, we don't need to put electrode array to the patient's brain to control the robotic limb. There is a new technology called targeted muscle reinnervation. which equals to repute a nervous system between robotic limb and your body that would let the robotic limb become part of your body naturally. When the patient wants to make some moves, nerve signals will still be communicated from the brain to the robotic limb, because the brain will not distinguish between the real limb and the robotic limb. And this new control system will make the robotic limb receive electrical signals, and after decoding , it will know what to do, just like real limbs.Rehabilitation Institute of Chicago, led the orientation of neuromuscular grafting technique compared to conventional prosthetic technology, which uses the electrode array, to have a very significant advantage. Traditional brain controlled mechanical limb in patients with brain implants require an analytical activity of the cerebral cortex of electronic equipment. This equipment may be rejected with the passage of time and the aging of the body. Also, the sensitivity and accuracy of the prosthesis will be unsatisfactory. Furthermore, to correct this problem, the patient doesn't need to go through surgery.
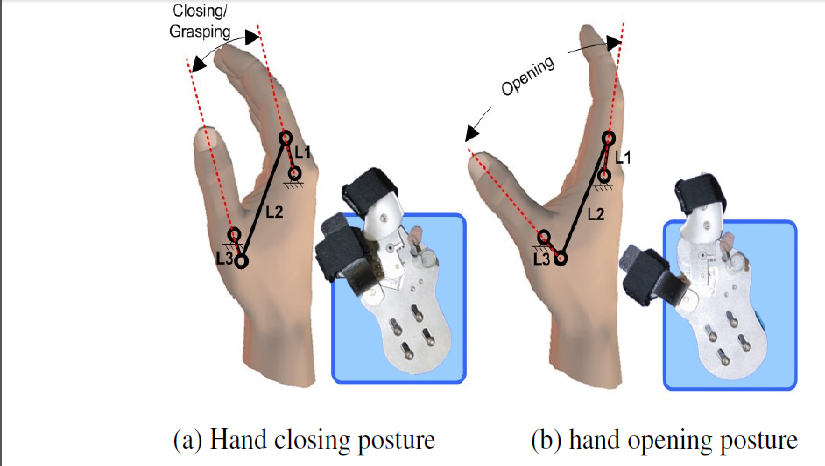
The most important part of building the limb is the DOF (Degree Of Freedom) that is built in the joints to help move the robotic limb. For the arm, there are 4 horizontal DOFs that helps in the flexion of the shoulder and 2 vertical DOFs in the glenhumeral joint of the shoulder. These DOFs are replaced in the glenohumeral joint to help keeping it in align with the shoulder. Therefore, the glenohumeral joint can move in all directions, backward and forward, up and down. Next, the hand's opening and closing is done by turning L1 (refer to the picture) to release the MCP joint (metacarpophalangeal joint) of all the fingers and L3 will be in charge of moving the thumb. this movement between L1 and L3 is the basis of opening and closing the hand. furthermore, the length of L1 and L2 can be changed depending on the texture of the objects that the hand is going to carry or hold.
Today, we don't need to put electrode array to the patient's brain to control the robotic limb. There is a new technology called targeted muscle reinnervation. which equals to repute a nervous system between robotic limb and your body that would let the robotic limb become part of your body naturally. When the patient wants to make some moves, nerve signals will still be communicated from the brain to the robotic limb, because the brain will not distinguish between the real limb and the robotic limb. And this new control system will make the robotic limb receive electrical signals, and after decoding , it will know what to do, just like real limbs.Rehabilitation Institute of Chicago, led the orientation of neuromuscular grafting technique compared to conventional prosthetic technology, which uses the electrode array, to have a very significant advantage. Traditional brain controlled mechanical limb in patients with brain implants require an analytical activity of the cerebral cortex of electronic equipment. This equipment may be rejected with the passage of time and the aging of the body. Also, the sensitivity and accuracy of the prosthesis will be unsatisfactory. Furthermore, to correct this problem, the patient doesn't need to go through surgery.
The most important part of building the limb is the DOF (Degree Of Freedom) that is built in the joints to help move the robotic limb. For the arm, there are 4 horizontal DOFs that helps in the flexion of the shoulder and 2 vertical DOFs in the glenhumeral joint of the shoulder. These DOFs are replaced in the glenohumeral joint to help keeping it in align with the shoulder. Therefore, the glenohumeral joint can move in all directions, backward and forward, up and down. Next, the hand's opening and closing is done by turning L1 (refer to the picture) to release the MCP joint (metacarpophalangeal joint) of all the fingers and L3 will be in charge of moving the thumb. this movement between L1 and L3 is the basis of opening and closing the hand. furthermore, the length of L1 and L2 can be changed depending on the texture of the objects that the hand is going to carry or hold.